
“We are all the wild things inside us which we do not need to fear because underneath is a powerful drive for care.”
An Interview with Dr Leo Russell by the Swedish Association for ISTDP. Reproduced with permission of Dr Niklas Lanbeck.
How did you get started doing ISTDP for functional neurological disorders?
During my psychology training I found myself frustrated to notice after “successful treatments” patients would often return with a completely new set of symptoms. There was something about the way I was working that was not reaching the deeper problems driving their difficulties. My supervisor at the time noticed my frustration and recommended that I read “Lives Transformed” by Patricia Coughlin and David Malan. This changed everything for me. I realised my own instinctive emotional repertoire was too limited to find the patient underneath and so I would need to learn this technique to help my patients achieve more lasting change.
I attended a summer school in Italy where I was blown away by the kindness and wisdom of the ISTDP community and teachers there. I was then fortunate to gain a place on ISTDP core training in London with Dr Rob Neborsky and Dr Josette ten have de Labije. It was the most wonderful experience. Even years later I regularly relisten to my supervisions from them both and I’m still learning from it to this day.
On core training both my teachers helped me to understand the relationship between internal conflicts, anxiety, defences and physiological symptoms. They were demanding for precision to detail and attention to building ego adaptive capacity so there were no short-cuts. I had to become much better at understanding the bodily experience of my patients. In one teaching block Dr Neborsky shared his clinical case “The Magical Mystical Medical Merry-go-round”. The classic case of a revolving door patient with extensive physical symptoms who had suffered iatrogenic harm from the medical system. It was so effective the way that Dr Neborsky worked with her and this transformed her life profoundly leading to a complete resolution of physical symptoms. This was the beginning of my interest in this area.
Dr Neborsky encouraged me to develop my interest in functional symptoms and after training helped me to co-author a paper on ISTDP for medically unexplained symptoms based on a case he had supervised. This paper also gave me an opportunity to collaborate with Dr Allan Abbass who was innovatively applying ISTDP in public healthcare settings, including for functional symptoms. He became a huge mentor to me and has given me so much guidance and support over the years. I don’t think there is a better schooling in ISTDP and functional symptoms than having the opportunity to have learned from Drs ten Have de Labije, Neborsky, and Abbass!
At the time I was working in complex mental healthcare for the UK national health service and, lo-and-behold, I discovered nearly all my patients had functional symptoms. I began to treat them with ISTDP, which became a victim of its own success. We ended up getting more and more referrals for people with functional symptoms which didn’t make me popular in a service looking to reduce referrals! Then the opportunity came up to work in a newly formed FND clinic in Exeter where I could focus on this group specifically. I had more fortune in the coming years as I also found a Neurology mentor Dr Steven Allder who was a great advocate for ISTDP in the field, and I had the opportunity to connect up with and learn from Dr Joel Town during his time working in Exeter.
During this experience I was able to co-author a number of papers with my mentors, first drawing on the data from Dr Abbass’ team in Nova Scotia and then later publishing data from our center in the UK. This culminated in a review paper with Dr Abbass and Dr Allder which was published in 2022. So that was how I got involved with FND, directly as a consequence of ISTDP.
Where were the patients coming from, would they get referred from somatic health care or also from mental health services?
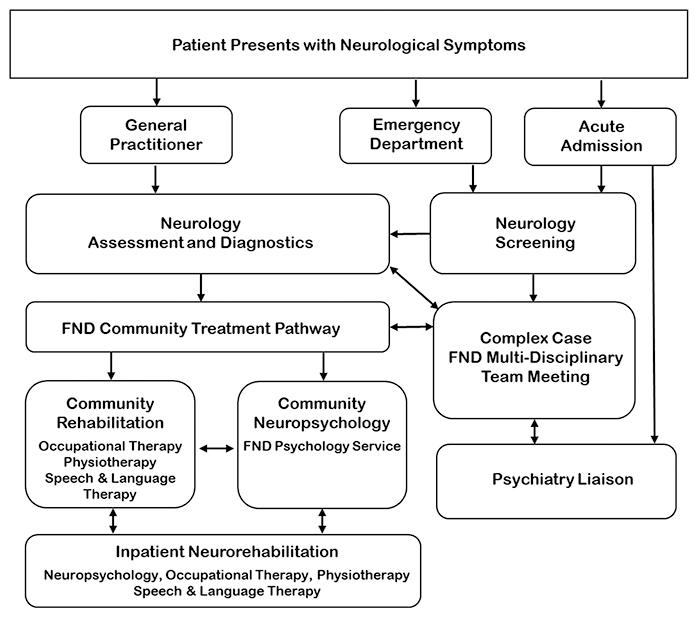
When I first joined, there were referrals coming from both the acute physical healthcare and the mental healthcare side. At that time there wasn’t really a clear pathway or diagnostic process. This was a problem because patients were arriving to see a psychologist when they felt their medical issues hadn’t been seriously assessed. No one wants to talk about their emotions when they are worried they haven’t had the right scans to rule out a brain tumour!
In the field of FND there is now quite a well developed diagnostic process in Neurology. One of the first things I implemented was to make sure that all patients who came to our service had first had an assessment from Neurology. Neurologists were expected not only to rule out other causes but to recognise FND profiles and talk to the patients about their diagnosis and the reason for referral to psychology. The patient didn’t have to completely be 100% certain it was FND, but they had to be in a position where they felt the neurologist had done the appropriate investigations and psychology was a reasonable next step.
{kind=link}
What’s your experience of dealing with the so-called barriers to engagement with this specific group of patients?
Well, I suppose there are two kinds of barriers to engagement. First are the patients you can’t get into the room with you and then second are the patients who are physically in the room but would rather be somewhere else.
For the patients who won’t see a psychologist we try and help them with their journey. We set up a multidisciplinary clinic in our pathway where we provided consultation to colleagues working with patients to offer formulation and guidance. We also had an excellent team of physiotherapists, occupational therapists, and speech and language therapists who not only do great work on FND within their own discipline but are often also terrific stealth psychologists too! It’s important not to respond to resistance at low rise of the unconscious alliance by being too directive. Instead we effectively just say to those patients who aren’t yet ready to come in the room by saying, “we’re here if you change your mind. You don’t have to see a Psychologist. There are other options”. Then sometimes these folks will find a way to psychology later down the line.
For that second group of patients who you can get through the door, that’s when ISTDP really comes into its own. Instead of doing an abstract formulation for the patient, you sit in the room, you do the emotion-focused interview, as Dr Abbass has described, and you see together with the patient if there is a relationship between their feelings, anxiety, defences and symptoms. The proof, as they say, is always in the pudding. Also, to extend the metaphor, we are careful not to over-egg the pudding. This process shows us if emotions are involved but it doesn’t rule out other contributing factors or causes. We say “this is one part of what might be contributing to your symptoms. Shall we see what we can do together about this?”
Having looked it up, not over-egging the pudding is a helpful image. The organisation you describeseems to be built around a high level of conscious alliance and this creates a platform for exploring symptom causation with the person?
One of the dilemmas in ISTDP terms is when patients are considering treatment, or when they first arrive for a conversation, they’re often at quite a low rise of unconscious therapeutic alliance and usually have poor ego capacity. From the off you might have projection or splitting coming with fear and hostility, patient confusion, regressive self-attack or acting out, or resistance with defiance and compliance. This is a recipe for disaster in standard medical settings. Doctors want to help and often it’s very painful when they don’t understand or when the patient is responding to them in confusing or upsetting ways. The whole thing can escalate and the medical system can act out and re-enact neglect, harm, and abuse.
We work with our colleagues, as you say, to build a platform for exploring symptom causation with patients. We work with patient advocates to support the system. We want all our clinicians to do their best to show patients they believe them, they know it’s not the patient’s fault, and that we have some options which might be able to help. Sometimes patients don’t take this up in the moment, but if they have a good experience they might choose to come back later down the line.
What about treatment histories and prior experiences of care, how does that affect the engagement phase?
Most patients won’t have received specific treatment for FND before and some have had no prior contact with mental health services either. The patients who haven’t received any psychological treatment often don’t know what to expect. I remember in particular the early days, some patients were genuinely half expecting that when they walked through the doors for psychology they would immediately be assessed as mad and then taken away by doctors in white coats.
That’s partly to do with projective processes but also to do with lack of understanding about what psychological treatment is. We try to embed a psychological strand to understanding FND across our multidisciplinary settings. When patients arrive they know what to expect and what not to expect. We also work closely with patient advocates and the charity FND FrieNDs which helps us to communicate better and reach patients who have fallen out with the medical healthcare system.
Patients who have more history of interacting with mental health professionals sometimes have more confidence in psychological treatment. It can be the other way too though, where they have less confidence, and over the years have attracted so many different diagnoses for all their related problems that they feel defeated. It can be helpful to work with these folks to see that their symptoms such as fibromyalgia, anxiety, depression, FND etc. aren’t necessarily different conditions they have to find different solutions to but they have related causes where helping one can also help the other. The first emotion a patient may be able to tolerate even a squeak of is a little bit of hope. This is often needed for chronic mental health patients who also have FND. Of course, you have to keep an eye out for the superego backlash, but this you can handle, once the hope has made an appearance the cat is out of the bag and you are on your way with the patient!
What do you think got us to a point where people think they will be declared mad? Like you said there are defences in operation but it also seems to latch on to something in our culture where emotional gets conflated with all in the head, made up, imaginary, simulated.
So there are lots of factors out there. One of these factors is that health services are still set up on dualistic terms. We have physical health services over here. And mental health services over there, but they’re in a different place. As if the mind and body are separate. So, no wonder our patients think that if there is nothing found wrong in their body causing their symptoms it means that they are losing their minds.
There’s also a complete lack of understanding about emotions in the real world. People think emotions are imposters that distract us from the good work of our rational brain. The public discourse is littered with stories of “crimes of passion” or “losing control of your emotions”. We have become very sceptical of feelings.
The field of Psychology has a major role in this. The behaviourists didn’t believe emotions had anything to do with human behavior. The cognitivists think that there’s no such thing as universal bodily emotions. They measured emotions by numbers and physiology and facial expression and concluded it could not be found. They never thought to just ask people about their feelings. This was deemed not scientific enough. Now the public perception of emotions is a complete mess. If our mental health professionals are confused and afraid of feelings then how can we expect our patients not to be?
Another element to this, certainly in the UK, is that health services are utterly overwhelmed. It is very painful for medical colleagues and healthcare professionals working with people when they feel they can’t help the person. The patient is flooded with emotional pain and anxiety and fear, the clinicians are overwhelmed with emotional pain and anxiety and guilt, and this creates a seriously combustible situation.
The clinician often avoid their confusion with false uncertainty and mad service boundaries, or they can act out by blaming patients or neglecting them or devaluing them, or they can burn out themselves which adds to the system’s resource problem. In this way we can tragically repeat a patient’s attachment history of insufficient or malevolent caregiving.
I think we see this a lot in psychiatry. It seems that for example neurologists might experience less destructive countertransference (“hate” if you will), because they get to say okay, not my table, off you go and best of luck. In mental health services if there are functional symptoms at a routine check it’s worrisome, interpreting it as functional might risk missing an organic cause but getting it assessed properly can be elusive, patients referred from psychiatry might not get access to adequate care. So there’s confusion and guilt and anxiety that pulls the relationship towards getting entangled or abandoned.
I completely agree. There are different ways that plays out. One way you have highlighted is risk of litigation. Neurologists deal with this too. I remember one of our colleagues misdiagnosed one patient, which is going to happen with such high numbers of patients even with a very low misdiagnosis rate. Afterwards, the Neurologist lost his confidence and started referring all his patients for unnecessary investigations leading to incidental findings and difficulty engaging patients in FND treatment. It came from a good place. He cared deeply about his patients. In the end he rebuilt his confidence but it took time.
When it comes to psychiatry it does depend on the psychiatrist’s training. It’s paradoxical because some of the most talented people working with FND, in my experience, are psychiatrists. At the same time psychiatrists in the UK currently don’t have to do any training in psychotherapy at all, so you have people starting out without any understanding of emotional processes in any form. When they face the patient’s unconscious and their own complex transference feelings are mobilised, they have very little to make sense of what is happening and they can feel terror or act out exactly as you describe.
It seems that the emotional and unconscious processes as causes of functional symptoms is often less controversial an idea in somatic health services. You’re going to present for us on the ISTDP theory of symptom formation in FND and you’ve written a paper on this in 2022. How is it generally received by colleagues who aren’t ISTDP practitioners when you present the theory?
For many colleagues when this is presented as one hypothesis amongst different possibilities which can be tested and is falsifiable there is really not a great deal of push-back. We all know in our own lives that we all experience functional symptoms to some degree or another. When I was taking health colleagues for trainings, I’d start the session by asking them if they could each sing one line of their favourite song in front of everyone else. Then you’d see anxiety and panic on their faces. I’d put them out of their misery and explain “I’m not really going to ask you to do that.” Instead, I ask them, “what happened to your body when I asked you that?” And they’d say, oh, my heart rate increased, or I got really hot, or I needed the loo immediately etc… Then I explain these are functional symptoms. A way that they are having real physical symptoms in relation to the current environment and their past experiences. Many people understood that intuitively. So I think coming at it from the common sense approach, which you indicate, was one way that people would accept it.
When I first started, I was so anxious, I think, to make sure that my colleagues knew there was a theoretical basis that was very solid for all this. I’d go in quite heavy on the theoretical background. They might have taken some of it in, but it was really only when I showed the videos of clinical work that colleagues would say, “I recognise this. I understand”. I learned the priority was to show, not to tell, and to start with the basics. So no major extended unlockings for newbies!
So again, the proof of the pudding is in the eating?
Exactly, yeah. The other part about the proof in the pudding is that within the field of FND there is a problematic history with psychoanalytic ideas in some quarters. Patients in the distant past have been genuinely harmed by people acting in the name of psychoanalysis. It was a product of its time and as such interacted with gender and power issues.
For instance, there was an idea that everyone who had hysteria, as it was called originally, had been sexually abused and this was now repressed in the mind. Either you found the repressed memories which proved the theory or you didn’t find them, which also proved the theory because they were repressed. I’m simplifying the narrative, but that is how it landed, and real harm was done. Our colleagues in the FND field are rightly protective of patients. First do no harm. It is incumbent on us to show them that what we are doing is not only effective but safe too.
One of the excellent patient advocates is known as FND Portal. He wrote this piece on “how did we get hysteria all wrong”. It’s offers an important perspective which helps us to understand some of the historical concerns with psychotherapies involvement in FND.
Very interesting! Nevertheless, this type of work does tend to uncover traumatic experiences, not typically repressed sexual abuse, but rather complex transference feelings from attachment trauma?
Attachment at its best helps prepare us for the slings and arrows of life, both psychologically and neurologically. At its worst, it is our first slings and arrows we face when we are not yet equipped to deal with them. The Ego Adaptive Capacity cannot develop and we are forced to respond to the world ‘as if’ we are always a moment away from existential obliteration. Our complex transference feelings can provide a way out, a way to energise the ego, but first we have to have the capacity to experience these feelings without becoming completely overwhelmed. Then when we experience the complex feelings we learn we are not the one dimensional monsters we see in our nightmares. We are all the wild things inside us which we do not need to fear because underneath is a powerful drive for care.
In the UK, what is the current status of ISTDP for FND?
First of all the UK is a great place to be practicing ISTDP. We have teachers and supervisors now trained by all the great leaders in the field from Davanloo and Malan to Neborsky, ten Have de Labije, Abbass, Coughlin, Frederickson and even more beyond that. Our home grown talents such as Alex Knowles, Sharon Lewis, Susan Hajkowski, Stephen Buller and Ross Crowther-Green have really driven the field forwards in this country with others making significant contributions to ISTDP abroad, such as Joel Town, Ange Cooper and Mark Stein! We have a pluralistic approach to ISTDP in the UK and a commitment to developing an evidence-base in public healthcare. My message to the ISTDP community is that the UK has a thriving ISTDP spirit and everyone is welcome! We would love to see you here!
In regard to ISTDP for FND we are well recognised by colleagues in the field. This has been helped by the work of Dr Abbass on FND and how he has developed good working relationships with FND leaders. I have delivered ISTDP teaching as part of FND Society Psychology programmes and recently we were also able to recognise ISTDP as one of the evidence-based models for FND in our British Psychological Society review on the psychological management of FND. The major reviews in the field recognise short-term dynamic psychotherapies as a joint leading model alongside CBT for people with FND (See Brown and Gutkin) and all the time there is increasing evidence for this approach. ISTDP colleagues, such as myself and Dr Javier Malda Castillo have been able to publish data on the efficacy and safety of ISTDP in the UK national health service specifically and this has also been well received.
What do you envision for the future?
I think we need to continue to work with colleagues in multidisciplinary settings to develop our understanding and knowledge of FND. We need to know what works for whom and when. We need to better understand which patients respond best to ISTDP and to find ways of integrating ideas from ISTDP in primary care settings so that patients can access support sooner. We need to get grants for larger multicentre studies in public healthcare and build on the existing evidence base. I am hoping that in the UK we can continue to work together and develop further links with our ISTDP colleagues doing great work across the globe in Canada, the US, Denmark, Sweden and beyond.
What do you think is needed to help people not trained in ISTDP or FND deal with these symptoms in their day-to-day work as healthcare practitioners?
This is a big question. First is an understanding of what FND is and what the experience is like for patients. Then is the understanding that FND requires a multi-disciplinary approach. Then we can begin to help people understand more about the relationship between the unconscious emotions, anxiety, defences, and physical symptoms. We also need to offer spaces for healthcare colleagues to process their experiences working with patients suffering with FND and other health conditions. We need to have real conversations in healthcare about the limitations of our resources and to confront the complexity of the task in helping people to recover. Too often in healthcare service we provide too little, leaving the patient and healthcare professional feeling like they have failed. Finally, better treatment pathways for FND need to be more widely implemented and this needs to be a joint venture across different levels of healthcare, beginning in primary care.
There’s a lot to gain for primary health care.
According to the royal college of general practitioners functional symptoms make up at least 20% of all GP appointments. In Canada, following on from Abbass’ work, Ange Cooper has developed an ISTDP-informed functional symptoms service within primary care to connect with GP surgeries, offering training for GPs to understand the triangle of conflict and pathways of anxiety. We need to do more of this. Often, GPs really get this stuff, they’ve got a lot of experience of these kind of symptoms, so with just a bit of help they can make a big difference. Ideally, we want to catch patients when they have maybe a little bit of pain, too much tension, or maybe a little bit of smooth muscle symptoms. We want to catch them at that point. Before it develops into IBS, or conversion symptoms, or losses of consciousness!
One of the things which increasingly I see a lot of in the UK is patients coming to the FND service, who two, three four years ago turned up in mental health services with depression symptoms or anxiety symptoms. Where the severity of their difficulties were not identified at that point and they were discharged without being offered a suitable treatment process. Perhaps just given some reading materials or something like that. And then the same people turn up two or three years later. But now, they’re more overwhelmed, their anxiety is more pervasive, their symptoms are more disabling and their neurological functioning is compromised. We need to solve this. Waiting until people get more ill is not a good option for a national healthcare system.
Do you think they would have had motivation to engage in therapy before the symptoms got that severe?
For some patients, for sure. The question is could they be helped to get to the point of meeting with a therapist and then could the therapist help build unconscious alliance through building ego adaptive capacity and mobilising complex transference feelings. Yes. I think that could happen.
We talk about different flavours of ISTDP and for fun I like to treat this as a concrete metaphor, as the edible equivalent to one’s therapeutic flavour. What would you choose to describe your flavour?
Haha. I’m a Neapolitan ice-cream kind of guy. The flavours have more in common than they are different. I’m just grateful for all the ice-cream makers that have made it so easy for me to eat my ice-cream. If I can, I do my best to add a little flake on top!